


QUICK LINKS: Practice Support Tools | Patients | Find a Neuro-Ophthalmologist | NOVEL | YONO Portal | Our Journal | Fellowships
Homonymous Hemianopsia
Patients: Download as PDF
Clinicians: Download as PDF
What is a Homonymous Hemianopia?
Homonymous hemianopia refers to an absence of vision towards one side of the visual world in each eye. The damage that caused this problem is in the brain and not in the eyes.
What is the anatomy of the visual pathway?
Many people are familiar with the concept that the left half of the brain receives sensations from and is responsible for movement on the right side of the body and vice versa. In a similar way, the left half of the brain receives visual information for vision from the right side of the world and the right half of the brain receives visual information from the left side of the world.
What may be the symptoms of a homonymous hemianopia?
- It is difficult to explain the sensation of a homonymous hemianopia. People with a right homonymous hemianopia often “feel like” the problem is in the right eye, but checking each eye by itself shows that the right side of each eye is affected. The same holds true for patients with a left homonymous hemianopsia.
- Affected people may bump into things on the side of the visual field defect. Driving may be particularly problematic: people may get into accidents as they change lanes because they cannot see oncoming cars or sideswipe objects on that side. Objects on a desk or table may not be seen on the side of the visual field loss, and sometimes even the food on that side of the plate is left uneaten. People need to be particularly careful walking through crowded places and crossing the street.
- Visual hallucinations may occur with homonymous hemianopia, especially if it develops suddenly as it would from a stroke. Affected people are often reluctant to mention this symptom but these are not related to a psychiatric disorder and may improve over time..
- Visual neglect describes a situation in which certain people with brain injury not only do not see to one side, but also do not even try to move their eyes and head to look to see what is on that side of the world. This increases the danger of bumping into things and getting into accidents. This is a problem related to visual “attention.”
- One may simulate what a person sees with a homonymous hemianopsia by showing a picture of a scene and then blanking half the scene as shown in Figure 1. The normal part of the brain may “fill in” the blank area with an extension of what it can see. Therefore, these people will not fully realize their problem.
Scene as observed by individuals without a homonymous hemianopia.

Scene as observed by individuals with a right homonymous hemianopia.

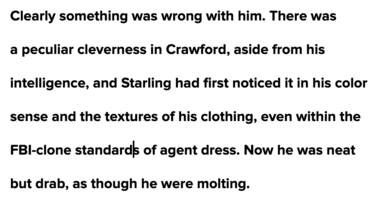
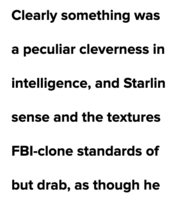
In another example, consider the following paragraph from Silence of the Lambs:
Real paragraph
Right homonymous hemianopia
How is a homonymous hemianopia diagnosed?
- A complete evaluation of the visual system is recommended. Often included in this evaluation is a visual field test that assesses for any visual field defects.
- Homonymous hemianopia may be caused by any disorder that affects the brain, including tumors, inflammation, trauma, but most commonly is due to a stroke in the occipital lobe, the most posterior part of the brain.
- Imaging of the brain by magnetic resonance imaging (MRI) is the most common diagnostic test used to diagnose the location and cause of the brain injury.
How is a homonymous hemianopia treated?
- Attempts to address the symptoms caused by a homonymous hemianopia may be directed at two areas: reading and dealing with the environment. Low vision specialists and vision rehabilitation therapists may be consulted to work on these techniques.
- Prisms or mirrors have been used on glasses to compensate for the blind field. These attempt to shift or relocate the visual world so that the vision within the defect is moved over towards an area of spared vision in one eye. These work for some but not all patients with homonymous hemianopia.
- More formal attempts to help recover visual field loss using computer assisted programs are controversial. These programs may not actually restore what is lost but instead retrain the brain to move the eyes more to “fill in the blanks” or pay more attention to their blind field.
- Some people can learn to make quick, often imperceptible eye movements toward the side of the homonymous hemianopsia. This allows them to quickly grasp information from the side of the visual world which cannot be seen. This adaptation can take months to develop.
What is my prognosis?
- Recovery depends on the underlying cause.
- The chance for significant recovery is lower after a stroke (blockage of blood flow to a region of the brain) than after inflammation or a mass has been removed.
Will my vision improve if I had a stroke?
- Any recovery that occurs is likely to begin soon after a stroke and reach its maximum improvement in the first 3 months and certainly by 6 months, with rarely any improvement occurring after that. If the underlying cause is not a stroke, the potential for improvement may differ. This should be discussed with your doctor.
Will I be able to drive?
- Driving poses a hazard for many people with homonymous hemianopia. Much depends on whether associated neurologic deficits are present, such as visual neglect.
- Many rehabilitation facilities have driving simulators both for training and for evaluating driving safety. Taking the driver’s test to allow an experienced examiner to assess driving safety may be helpful.
- Vision requirements for a license to drive may be found for individual states on the Web. Most states do have a minimum visual field driving requirement. If you have any doubt about whether your visual field loss disqualifies you from driving in your state, ask your doctor and check with your state’s DMV office.
Copyright © 2023. North American Neuro-Ophthalmology Society. All rights reserved.
This information was developed collaboratively by the Patient Information Committee of the North American Neuro-Ophthalmology Society. This has been written by neuro-ophthalmologists and has been edited, updated, and peer-reviewed by multiple neuro-ophthalmologists. The views expressed in this brochure are of the contributors and not their employers or other organizations. Please note we have made every effort to ensure the content of this is correct at time of publication, but remember that information about the condition and drugs may change. Major revisions are performed on a periodic basis.
This information is produced and made available “as is” without warranty and for informational and educational purposes only and do not constitute, and should not be used as a substitute for, medical advice, diagnosis, or treatment. Patients and other members of the general public should always seek the advice of a physician or other qualified healthcare professional regarding personal health or medical conditions.







.png)

_250x90.png)